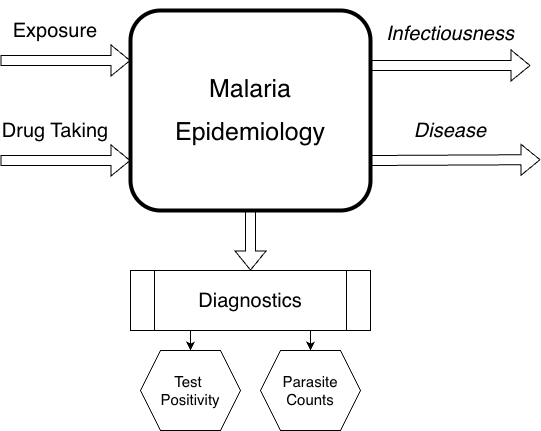
Human Malaria Epidemiology
Exposure, Infection, Disease, Immunity, Infectiousness, Diagnostics and Detection

Mathematical models of human malaria are based on some understanding of the basic biology. In malaria policy, the models…
We define human malaria as any disease caused by infection with malaria parasites. Here, we are focused on the study of Plasmodium falciparum epidemiology using mathematical models, including infection, immunity, disease and related topics. In most cases, the term malaria model means that the state space for the vertebrate host model component of a model has features that are meant to resemble malaria.
In this essay, we outline our approach to building malaria models that we can rely on for malaria analytics. We don’t need the model to be perfect, but it ought to be – in words I learned as a farm hand – pretty damned good (PDG). This essay thus has four sections:
Introduce the challenge of Building a Malaria Model.
Introduce the simple models that are building blocks for malaria models that we can rely on.
Discuss some mathematical techniques that can be used to handle both age and time
We introduce some PDG Malaria Models
Building a Malaria Model
To build a malaria model, we must ask a few basic questions. If we start with the basic mathematical epidemiology of malaria:
What are the essential, disinctive features of malaria infection and immunity?
To avoid delving too deeply into aspects of malaria that are primarily of academic interest, we must also ask:
What features of malaria are essential for evaluating malaria policies?
Overall, malaria is a unique combination of features. A common starting point for malaria is thus the SIS compartment model. Malaria immunity tends to be weak, so it is sensible to assume that individuals will become susceptible after clearing a parasitic infection. If malaria induced protective immunity after a single exposure, then we would start (instead) with an SIR model. Malaria parasites replicate in humans: if malaria did not replicate in the host, we might choose to start with a macroparasite model.
Malaria infections can last for several months: some people have carried infections for decades. Because malaria infections last a long time, malaria metrics are developed around malaria prevalence. A study of malaria diagnostics and detection thus plays a central role in the mathematical study of malaria.
The representation of malaria biology using mathematics present several challenges: how to handle superinfection and the complex time course of an infection; how to build an accurate state space for infection and immunity; how to model disease; how to handle age and time; and how to handle the overwhelming complexity. We want malaria models of intermediate complexity that are good enough to address the policy questions we confront.
How do we get there? To get there, we start with studies that have explored malaria thematically and developed a set of building blocks.
What do these building blocks do for us? Since infections last a long time, when malaria exposure is high, a single person can get superinfected, and models often look at the multiplicity of infection. Models for superinfection start with a queueing model called M/M/\(\infty\) that work a lot like macroparasite models, but they are very difficult to extend. We frown on SIR models – a recovered and immune state almost never follows exposure – but models with stage structured immunity have some nice features, so it would be better to use those. These stage structured models, and most of the supporting evidence, suggests that immunity accumulates with age and exposure. We need models that track infection status by host age over time, but we want to avoid the practical computational challenges that come with partial differential equations or individual-based simulation models. On top of this, we need to consider disease, drug taking, vaccines, and infectiousness. If we try to put all this into a compartment model, we bump up against a real challenge: as we combine features (host age, multiplicity of infection, stage of infection, stage of immunity, chemoprotected, vaccinated), the number of states explodes combinatorically. As we review the building blocks, we’ll come across hybrid models, that set the stage for using tracking variables that make it possible to manage some of the complexity.
Building Blocks
Some of the models developed for malaria focused on specific aspects of malaria, and these studies have developed a set of building blocks. In the first part of this section, we present models that focus on features:
exposure to malaria through the bites of infectious mosquitoes;
infection - the complex time course of an infection; the duration of a simple, untreated infections; superinfection
age of infection
stage of infection
multiplicity of infection
hybrid models
immunity and effect modification, including models with stage-structured immunity and exposure tracking variables
stage-structured immunity
exposure tracking
disease the relationship between exposure, infection and any disease including fever, anemia, & severe disease
diagnostics & detection play an important role in clinical and research settings
models of treatment with antimalarial drugs that cures infection and provides a brief period of chemo-protection
drug taking rates
adherance
malaria vaccines
Age & Time
Next, we discuss the problem of handling age and time. In developing most models, we will treat them as models for cohorts of humans as they age.
PDG Malaria Models
For malaria analytics, the standard is fit for purpose. Lives are on the line, so we need models that are accurate enough to rely on. We don’t need the model to be perfect, but it ought to be – in words I learned as a farm hand – pretty damned good (PDG). For malaria analysts, we will restrict our study to models that can be built and solved in a reasonable amount of time, so we will largely steer clear of individual-based models. The last section describes some PDG malaria models.