
Welcome to The UW Shoulder Site @ uwshoulder.com
Please note that information on this site was NOT authored by Dr. Frederic A Matsen III and has not been proofread or intended for general public use. Information was intended for internal use only and is a compilation for random notes and resources.
If you are looking for medical information about the treatment of shoulders, please visit shoulderarthritis.blogspot.com for an index of the many blog entries by Dr. Frederick A Matsen III.
Exactech Proximal Humeral Fracture Repair Technique Guide

Setup
Ensure that you do a good job of inspecting the skin of the extremity you are repairing for open lesions. Also inspect the axilla for Candidal lesions
Place templated x-rays, clinic notes and progress note on x-ray box.
Prefill-out orders and setup pt in a beach chair position. The operative arm should be able to hang off bed as shown below.
.png)
.png)
You should circumferentially wrap cloth tape around the patient's chest and table to prevent pulling the patient off of the table during the surgery. This taping is in addition to use of the patient's normal safety belt.
DO NOT REMOVE THE SHOULDER SUPPORT! Removing the shoulder support under the operative side may seem like a good idea but the patient will eventually migrate off of the table and can, and have fallen off the table in the past.
The anesthesia team and ortho team should work together to tape the patient's head down. You may need to use a clipboard to suport the head. We do not secure the head in a brace as shown above.
A 1010 drape should be secured around the patients neck and the free end secured to the tape holding the patients head. Securing the free end prevents it from falling onto the sterile field when prepping.
ROM of the operative shoulder should be measured and recorded on the board in the following order: FE, ER, IRA, ERA, CBA.
Double Prep
A member from the ortho team needs to wash and gown and prep the patient's operative side. Iodine is the prep of choice.
Prep from the middle of the chest out to the wrist, followed by armpit, followed by wrist, hand and fingers. This should be done a total of three times.
The first drape is setup under the patients head, operative arm and over the patient's waist. If possible, the drape should be tucked under the patient's belt. This draping is done by the nursing staff or other member of ortho team.
The first set of gloves are removed and the second prep is performed in the same manner as the first.
The second drape is setup over the first in the same manner.
Draping
After the two initial drapes are placed under the head shoulder and over the waist, one drape is place over the chest and feet. This should go from the patient's armpit to the patient's neck.
Another drape is placed over the head and overlaps across the chest drape.
The three corners where these drapes come together are stapled. There is no need to staple the drapes directly to the patient.
The arm should be covered with a stockinet and a dry sponge placed in the patient's axilla.
The primary surgeon will mark the coracoid and a line from the coracoid down the delta pectoral interval. This interval can and should be palpated prior to marking.
A clear adhesive plastic is used to cover all exposed skin.
At some point a timeout will be performed by the circulating nurse, attending and anesthesia team. The room should otherwise be free from any talking or other distracting noises during the timeout.
Approach
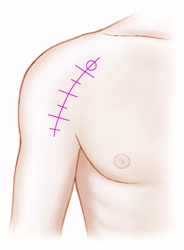
Make your incision from the coracoid down 10 or so cm.
After incision through the dermis, two interposing gelpi retractors should be used to separate the two skin edges and to pull them away from the muscle bed.

A scalpel should be used until the surgeon reaches muscle. Mayo scissors are then used to dissect through fascia to locate the cephalic vein and delta-pectoral interval.
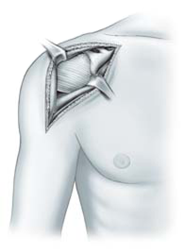
The delta pectoral interval should be blunt dissected with the surgeon's index finger, taking the vein laterally. Make an effort to preserve as much deltiod muscle as possible.
The motion interface under the deltoid and pectoralis should be freed up and the conjoint tendon located.
Remember to free up the conjoint tendon on its lateral side so that the tendon can be pulled medially. Incising into anything medial to the lateral border of the conjoint tendon can result in median nerve injury.
When the lateral border of the conjoint is freed up, use a medium Richardson retractor to pull the conjoint medially. Use a Balfour to expose the rotator cuff /superior humerus.
Bursa should be removed to better visualize the subscapularis and humerus. Locate and identify the bicipital groove.
Humeral Head Inspection
Inspect the humeral head and assess the fracture. It may be necessary to fracture the head at the bicipital groove.
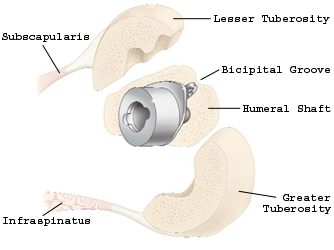
Use three number 5 Tevdex to tag the Greater and lesser tuberosities. These will be used to retract the larger bone fragments to allow for better exposure to the glenoid and shaft. Later, they can also be used to pass suture or be passed through the prosthesis for tuberosity tie down.
The articulating surface of the humeral head will need to be removed to allow space for the prosthetic head. Save all bone for bone grafting later in the case.
Determine the approximate size of the shaft according to the templated xray. Assess the size of the humeral shaft to determine if this size seems appropriate.
Humeral Shaft Prep and Prosthesis Size Determination
Ream the humeral shaft with the proper sized reamer. Reamers are 1 mm larger than the size of the prosthesis to allow for a 0.5mm cement mantle.
Prostheses come in size 7mm, 9.5mm and 12mm. Reamers come in size 8mm, 10.5mm and 13mm.
You may need to start with the smallest reamer and work your way up. The shaft should not be overreamed.

Trial the component.
Ensure that you are using the proper side by ensuring the lateral dorsal fin matches up with where the bicipital groove is expected to be. Of note, the trial stem has been enlarged to simulate a 50mm cement mantle (1 cm greater diameter).

Use the impactor tool shown below to help position and drive the trial into the humeral canal as needed.

A trial reduction tool is provided in the Exactech kit, but will not likely be used by our service. These are specific to each size of prosthetic trial component and the label of the side (Right or Left) should readable when placed anteriorly against the humeral shaft.

If used, it should be centered on the shaft and K-wires are used to hold this in place.

After the proper prosthetic size and version have been selected, determine the height position of the prosthesis by adjusting it to the tuberosities.
Now determine the head height and position Then trial your head and pay particular attention to the position of the head in relation to its eccentricity.
Use the patient's head to determine the approximate humeral head size you will need. Note that all heads larger than 41mm have a 1.5mm offset.

Heads come in three heights: Short, Tall and Expanded.
| Head Size | Short Head | Tall Head | Expanded Head |
| 38 | 16 | 19 | |
| 41 | 16 | 20 | |
| 44 | 17 | 21 | |
| 47 | 18 | 22 | 26 |
| 50 | 19 | 23 | 27 |
| 53 | 20 | 24 | 28 |

After the correct shaft and head combination has been selected, the shaft should be prepared for cement and with suture. Do a good job of washing the shaft out and testing the bottom of the medulary canal. If no bottom is noted, the shaft should be rereamed or fitted with a cement plug.
Two holes should be drilled with one on each side of the bicipital groove for your "North-South" sutures.

Run two number 5 Tevdex through your holes and clamp them off.

Suck out the shaft and place a vag pac in the canal.
The actual prosthesis should be assembled with attention to positioning of the eccentric head. Impaction of the head is accomplished by placing the prosthesis vertical on two folded green towels. One person holds the prosthesis firmly, while a second person holds the impactor and give three good blows to the impactor with a mallet.
![]()
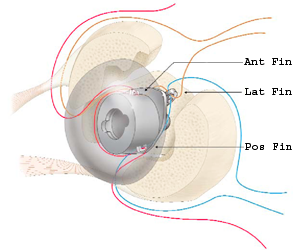
PreThreading the Prosthetic Fins
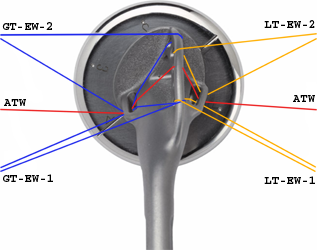
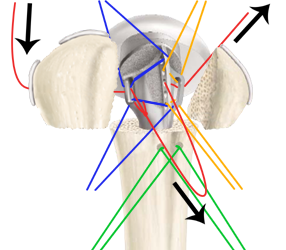
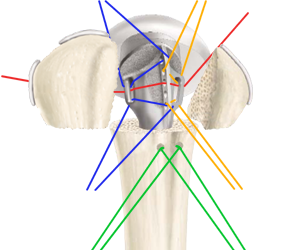
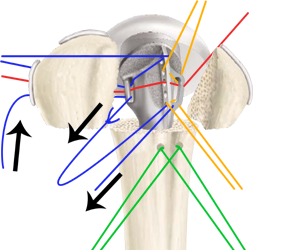
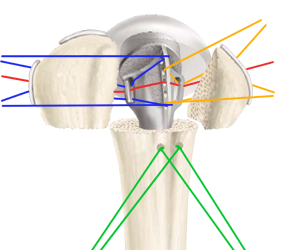
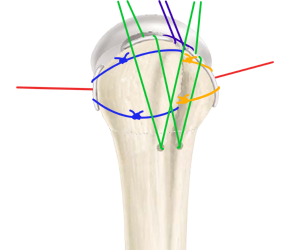
You will want to place a number 5 Tevdex suture through each of the prosthetic fins as shown below. This will be used as the final cerclage (FC), AKA "Around-The-World" (ATW) tie.

The the anterior and posterior prosthetic fins will need 2 number 2 Tevdex sutures placed through each of them and through the lateral (dorsal) fin as shown below. Number 2 Tevdex is used to help identify them from the number 5 Tevdex "Around-The-World" pull suture. These will be used to pull the greater tuberosity (GT) and lesser tuberosity (LT) into the prosthesis. These may be referred to as GT and LT horizontal or "East-West" sutures. Clamp off our suture ends so that they don't come undone during impacting of the prosthesis.
Note: The surgeon may wish to pass the "Around-The-World" and/or the Great Tuberosity "East-West" sutures through the infraspinatus prior to cementing of the prosthesis.
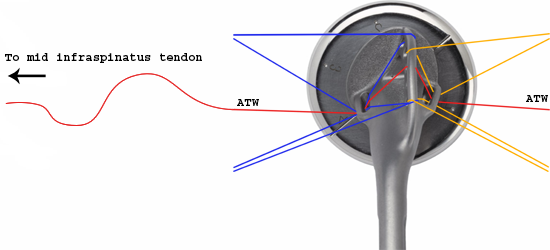
Optional technique
Cementing
One packet of Simplex cement is mixed with two grams of Vancomycin and loaded in a Caulk Gun with a narrow applicator.
The vag pac is removed from the shaft and the canal receives its final suctioning.
The humeral canal is cemented from the bottom of the shaft so that the pressurized cement forces the cement applicator out of the hole. Excessive cement is removed.
The prosthesis is positioned in the correct version and pressed in as much as possible and impacted with an impactor until the proper height is achieved.
![]()
Excessive cement is removed with a Joker and/or periosteal freer. Check the version again and wait for the cement to harden.
After the cement becomes hard, the shoulder should be inspected and extra cement removed.
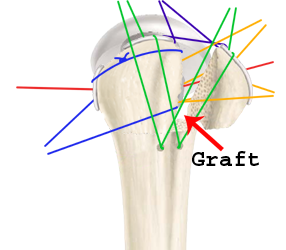
Placement of Ties
All ties should be passed through their respective paths and clamped off prior to tying. This does not need to be done sequentially.
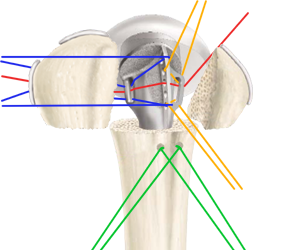
You should have 1 number five Tevdex and 4 number two Tevdex sutures threaded through the prosthesis and 2 number 5 Tevdex through the holes made in the humerus.
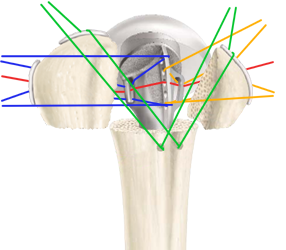
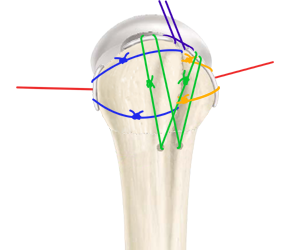
You you have not run the posterior end of the "Around-The-World" suture through the middle of the infraspinatus, you will need to set this up now. Either pass a number 5 Tevdex through the middle of the infraspinatus, or use one of your tag stitches as your tie. With the posterior free end of the "Around-The-World" suture, tie a half hitch around the deep end of your free number five suture.
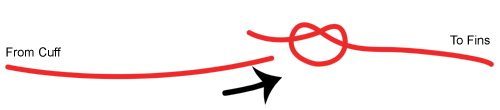
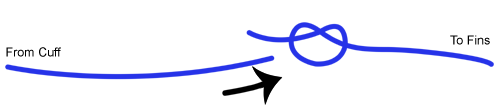
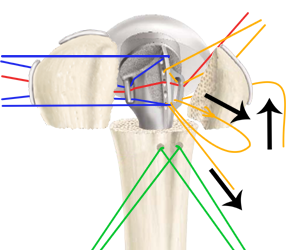
After you tie your pull suture around your cuff suture, carefully pull them through each fin, one at a time so that the new number 5 cuff suture goes through the infraspinatus and all fins of the prosthesis (as shown below).
Around-The-World pull suture pulling suture from cuff through fins
Camp off this suture.
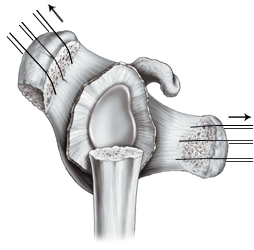
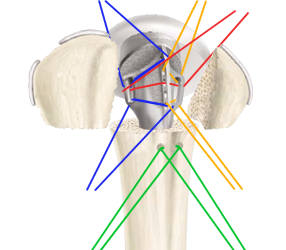
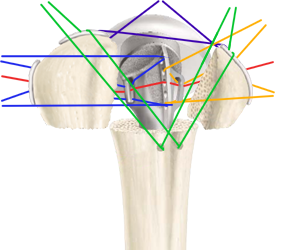
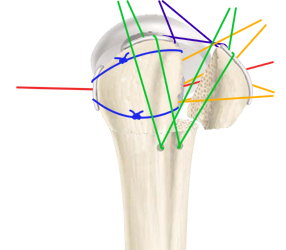
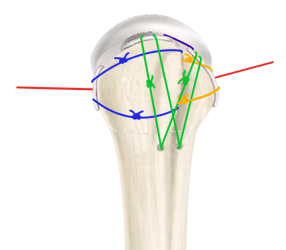
If you did not pre-thread your Greater Tuberosity "East-West" through your infraspinatus tendon, you will need to do this now. Either pass two number 5 Tevdex sutures through the superior and inferior portions of the infraspinatus, or use your tag stitches for your ties. With the posterior free ends of the Greater Tuberosity "East-West" sutures, tie a half hitch around the deep end of your free number five sutures.
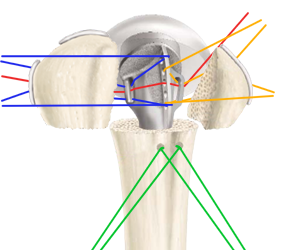
After you tie your pull sutures around your cuff sutures, carefully pull them through each fin, one at a time so that the new number 5 cuff sutures wrap around the infraspinatus, posterior fin and lateral dorsal fins of the prosthesis (as shown below).
Camp off this sutures.
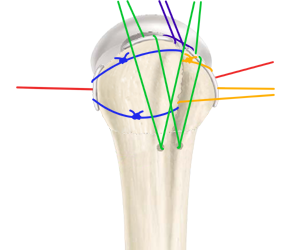
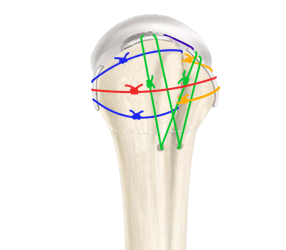
Either pass two number 5 Tevdex sutures through the superior and inferior portions of the subscapularis, or use your tag stitches for your ties. With the anterior free ends of the Lesser Tuberosity "East-West" sutures, tie a half hitch around the deep end of your free number five cuff sutures.

After you tie your pull sutures around your cuff sutures, carefully pull them through each fin, one at a time so that the new number 5 cuff sutures wrap around the subscapularis, anterior fin and lateral dorsal fins of the prosthesis (as shown below).
Camp off these sutures.
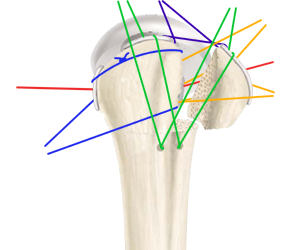
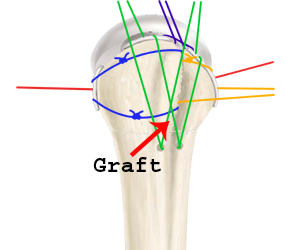
Pass the anterior "Around-The-World" suture through the middle of the subscapularis. If is it not easy to pass on its own, use a tag stitch or pass a number 2 Tevdex suture through the subscapularis and use this to pull the anterior free end of the "Around-The-World" suture through the subscapularis tendon. Clamp the free ends of this suture together.
Run the "North-South" sutures through their respective suprspinatus and superior subscapularis tendons. Clamp them off.
Run a separate number 5 Tevdex through the anterior supraspinatus and superior subscapularis so that the free ends exit the inner surface of the cuff muscles (as show below). This is your Rotator Interval tie and you will later want your knot to be on the undersurface of the tendons. Clamp it off.
Make sure that you have all of your sutures set up and prepare to tie.
Tying
After you have double checked that all sutures are set up correctly, it is time to start tying. This must be done sequentially to achieve the best fixations of the tuberosities around and through the prosthesis.
Fist tie down down the superior GT "East-West" horizontal tie.
Then pack the space between the greater tuberosity and prosthesis full of bone graft.
Tie down the inferior GT "East-West" horizontal tie.
Fist tie down down the superior LT "East-West" horizontal tie.
Then pack the space between the lesser tuberosity and prosthesis full of bone graft. Make sure you have a good amount of graft in the opening between the dorsal fin and body of the prosthesis.
Tie down the inferior LT "East-West" horizontal tie.
Tie down the GT "North-South" and LT "North-South" vertical ties.
Then tie down the rotator cuff interval tie, ensuring that the knot is buried under the cuff. Placing the knot on top of the cuff can create an irrigating lump and a source of future problems.
Tie down the "Around-The-World" tie.
Use bone graft to fill in any open spaces as needed and add additional ties as needed. Knots should be buried if possible and the outer surface of the humeral head should be free of significant protrusions.

Closing
Close the delta-pectoral interval loosely. Emplace a drain over deltoid and exit skin a good 7.5cm or more away from incision site. Use staples to close the wound.
Skin should be cleaned with alcohol to remove any residual iodine.
Postop
No CPM
Place Pt in sling
For PT - Axillary care and hand to mouth exercises.
2 view Xrays immediately post op - AP Grashey and Axillary

