
Information + health
I was born in 1980 at a hospital in rural Oregon. As is still current practice, the staff overseeing my birth peeked at my anatomy, and checked “male” on my birth certificate. For the next 38 years, this one bit of binary health data was the basis for a profound number of experiences in my life. It was entered on forms registering me for public school. My pediatricians used this bit, without ever actually inspecting my body, to shape their preventative health care decisions about my weight, mental health, and risks of eating disorders. And when I turned 18, the government used this bit in its decision to send me U.S. military draft card. This single bit of binary data, far more than my body, shaped the course of my childhood and adolescence, both in health care and beyond. And, of course, I wasn’t a boy, or a man; as a transgender person, that bit was wrong, and it ended up defining more than how people treated me: it ended up defining how I saw myself in devastating ways.
Racing forward to my late thirties, I finally fixed that bit, correcting my birth certificate, health records, my government identification. And because in health care, it more often data that drives decisions, the health care system now treats me as the woman that I am. There’s just one problem: because health information technology is still binary about gender, it leaves no room for the sexual and gender diversity. I have a prostate gland, but I no longer get reminders about prostate exams, and my doctors no longer ask. I do not have a cervix, but I regularly get urgent reminders about overdue pap smears. Physicians unfamiliar with my trans body ask my why I don’t have a gynecologist and I get confused stares in the lobbies of urologists. And when I ask providers about gender-influenced health concerns about heart disease, kidney stones, osteoporosis, and strokes, they either shrug, and say, “There’s no science on your trans body” or they just assume the binary science on gender difference applies, treating me like every other woman.
These experiences, far from being about transgender health alone, reveal the complex interactions between health and information. Data about health is often used as a proxy for our anatomy and physiology, and when that data is biased, it biases care for our health and wellness. Data about our bodies, whether it’s carefully measured or simply assumed by someone looking at our bodies, is used to inform decisions outside health care, in education, work, and government. And science about health, which is our primary guide in shaping health care, is only as good as the data we collect. In the rest of this chapter, we will survey these complexities, mapping their interactions across different scales of our bodies, our selves, our health care systems, and our communities.
DNA as Information
In one sense, all life on Earth is partially influenced by information stored in DNA. First discovered in 1869 by Swiss chemist Friedrich Miescher, it was first called “nuclein”, as it was found in the nuclei of human white blood cells 14 . As its chemical structure was studied further, it was renamed “nucleic acid”. Only after hundreds of research papers later did scientists discover the three major components of a single nucleotide (a phosphate, a sugar, a base), and the carbohydrate components of RNA and DNA (ribose and deoxyribose). No one yet knew how these components were arranged spatially; it wasn’t until Erwin Chargaff, inspired by a major discovery that genes are composed of DNA, launched a research project to understand the structure of DNA, finding that no matter what DNA his team sampled, there was a consistent volume of adenine and thymine, and consistent volumes of guanine and cytosine. This realization eventually led to James Watson and Francis Crick’s use of 3D modeling, first advanced by biochemist Linus Pauling, which led to the famous discovery of the double-helical structure of DNA. This nearly 100 year history of science culminated into a single profound fact of nature: all life that we have observed thus far, is encoded as long sequences of AT, GC pairs, stored in nuclei, used in cell replication. This information, repeatedly replicated more than 30 trillion times in our bodies over our lifetimes, is the basis of our reproduction, of evolution, and often our deaths 15 .
The discovery of DNA has had profound effects on the science of life. For example, biology shifted a discipline of subjective description and classification to one of data analysis. This practice, now called bioinformatics , entails using machines to sequence DNA, algorithms and statistics to analyze DNA sequences, and the broader science of genomics to understand the particular sequences of DNA that contribute to disease 1 . For example, one branch of bioinformatics investigates the parts of DNA that, when mutated through our bodies’ imperfect process of DNA replication, tend to lead to cancerous cells, which tend to ignore critical signals that stop cell division, while also being able to evade our immune systems, and consume resources from blood vessels that other normal healthy cells need. This work is beginning to shape medical practices, helping us detect biomarkers that correlate highly with cancer risk 19 .
Understanding DNA as data also led to the record fast production of the SARS-CoV-2 vaccines in 2020. The virus, first detected by Chinese scientists, was known to have a distinctive “spike”; they quickly sequenced the 29,903 bases of its RNA and shared it globally on January 10th, 2020, just one month after the first identified case. Hundreds of scientists, using methods of bioinformatics, quickly determined that its RNA sequences were very similar to a previously known virus, SARS, another coronavirus. This led to the name SARS-CoV-2. German virologist Christian Drosten, who had long studied coronaviruses , developed the first test for this virus a few weeks later, by detecting particular bases in the virus’s genome. And then, using technology from the 1990’s to create mRNA vaccines that would inject instructions for human cells to producing the innocuous coronavirus spike, Pfizer and BioNTech partnered to construct the first vaccine in just a few weeks. The vaccine, essentially a sequence of RNA wrapped in a fatty acid, teaches our cells how to build the spike, which triggers an immune response that teaches our body to recognize and attack the full virus. The next 6 months involved clinical trials to verify the efficacy of the vaccines. None of this would have been possible, especially so fast, without understanding that DNA and RNA are essentially data. (Nor would it have been possible without decades of public investment in basic research by governments around the world, especially the United States and China.)

Health research as information
How do we know that a vaccine works? Or that any health care practice works? This knowledge, and the processes by which we produce it, are the foundation of modern medical practice. But for most of human history, we lacked this foundation 2 . Physicians had practices that were grounded in faith or superstition. For example, bloodletting was a practice of intentionally removing blood from patients to cure illness and disease, under the theory that blood and other fluids were “humours” that, when in proper balance, would maintain health; removing blood, therefore, was one way to restore “balance”.
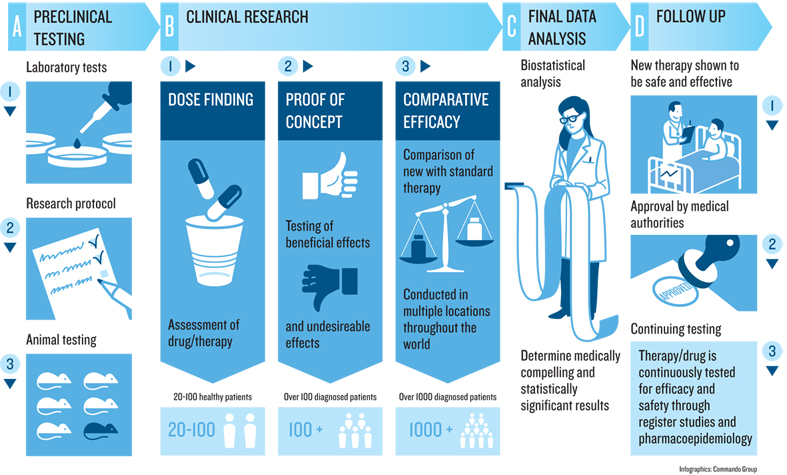
These superstitious practices began to shift in the 18th century. In 1747, physician James Lind was trying to address scurvy amongst sailors; amidst the backdrop of the broader scientific revolution of the 18th century, he decided to compare 12 similar patients, dividing them into each given different groups, and giving each different treatments. The ones who were given oranges and lemons were the only ones that recovered quickly led to the first evidence of scurvy as a vitamin-C deficiency. This was one of the first examples of a controlled experiment , or what health sciences usually calls a clinical trial .
The practice of clinical trials advanced from there. In 1811, the first documented use of placebos occurred, using deception to give a treatment that is known to be ineffective, but present it as the treatment being tested. In 1943, the first double-blind trial occurred, ensuring that both the patients and the providers giving treatments, were not told whether the treatment was a placebo. In 1946, the first randomized controlled trial occurred, in which the assignment of patients to the placebo or treatment group was random rather than self-selected or provider selected. All of these improvements, and the countless others that have followed since, have greatly increased the confidence and certainty of the methods by which scientists deem interventions to be effective. And this entire history of producing knowledge was brought to bear in evaluating the SARS-CoV-2 vaccines, to the point where universities and companies have well-established procedures and infrastructure, government units like the U.S. Food and Drug Administration have well-established regulations for evaluating clinical trial results, and medical journals, read widely by medical providers, have well-established norms for objectively reviewing and publishing the results of trials.
While clinical trials are the highest standard in producing knowledge about health interventions, there are countless other research methods used to build knowledge about health and medicine. Descriptive studies can identify new phenomena and theories about health. Correlational studies,—like the kind often reported in journalism indicating that eating some food increases or decreases the risk of some disease—can help generate hypotheses to be later tested in randomized controlled experiments. And qualitative methods, such as interviews, field observations, and ethnographies, can help identify social, cultural, and organizational factors that shape the efficacy of interventions. For example, it doesn’t matter if a drug is effective if someone doesn’t take it correctly, forgets to take it because of a complex dosing schedule, or did not keep the instructions on how to take it because they are homeless. Qualitative methods shape our understanding of why a medication does or doesn’t work, as the reasons are often sociocultural, not physiological.
Regardless of method, the same values, biases, and systems of oppression that affect all data, information, and knowledge, affect health knowledge, resulting in science that supports and highlights the experiences of dominant groups, while often disregarding or erasing the experiences of marginalized groups, or even doing direct harm. For example, a study conducted between 1932 and 1972 of syphilis recruited Black men, telling them that they were receiving free health care from the federal government. The reality, however, was that the government study was observing the natural course of syphilis, and administered no care when it was detected, did not notify the men that they had detected it, and even offered placebos that were known to be ineffective. As a result, hundreds of men died of syphilis, forty partners contracted the disease, and 19 children were born with congenital syphilis. The focus on Black men was explicitly racist 3 , and the lasting generational impact has been a pervasive distrust of medical science amongst Black Americans 6 , further introducing racial bias into the scientific foundations of health care knowledge. This recent history—recent because there are many Black Americans who were participants in this racist exploitation, or whose parents were—has undergirded reasonable skepticism in some Black communities about the safety of COVID-19 vaccines.

Information in health care
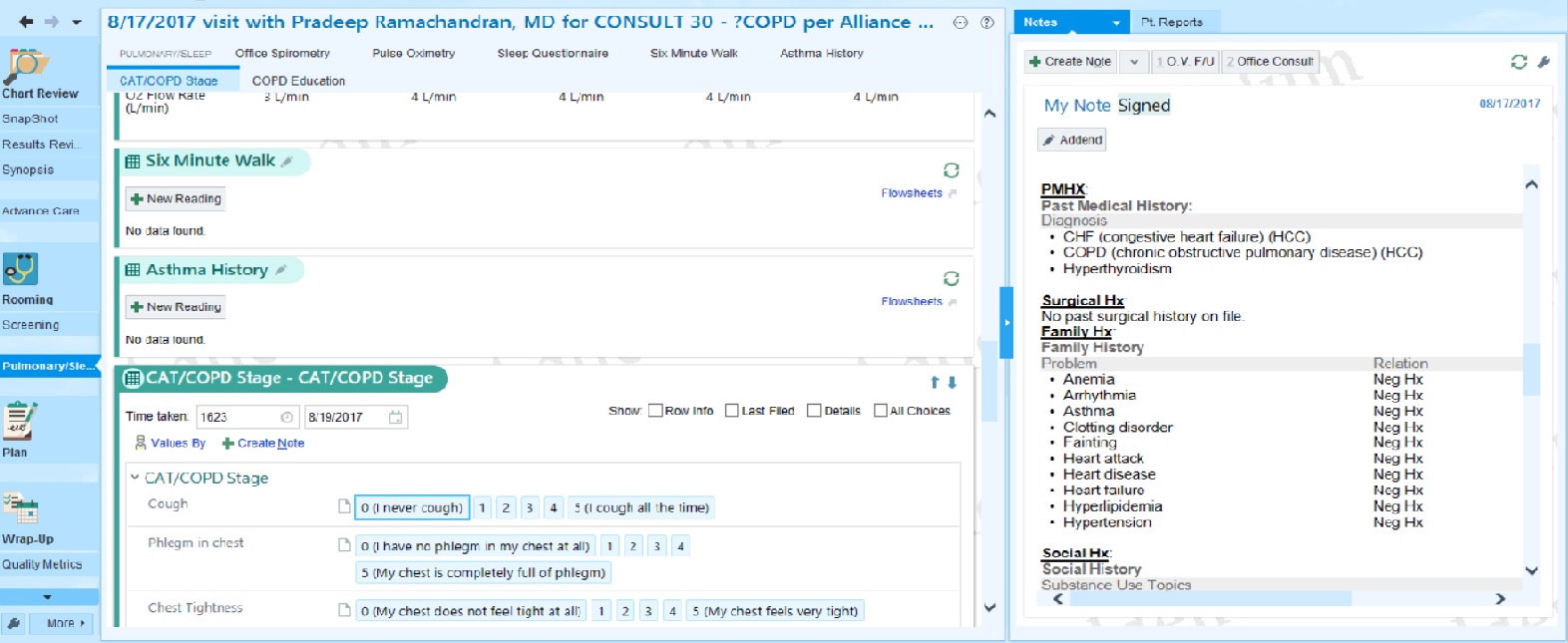
From both a patient, modern health care is rife with information problems. When we experience symptoms in our health, we rely on information from friends, family, and increasingly the internet to even decide whether to utilize health care services 17 . When we visit health care providers, we often first interact with medical assistants, who take vital information from our bodies such as our weight, blood pressure, and heart rate. Conversations with physicians are often centered on gathering information about our experiences, including pain or other symptoms, the duration of symptoms, and if they are mindful of social determinants of health 10 , the context of our lives that may be causing or aggravating these systems. If conversation is not enough, providers may order more systematic tests, measuring properties of our blood, stool, urine, bones, skin, and more. All of the information that providers gather goes in medical records, now mostly electronic like the one above, as a central database for data about our anatomy, physiology, and its change over time. And if provider and their team can make a judgement from this information, whether a diagnosis, or some next step for gathering more information, they communicate that to us as information, often giving us printed materials to read, medications to take, or other home remedies to follow, all with instructions that attempt to translate a medical judgement into something we can comprehend and follow.
Of course, the information-driven processes above are rarely so seamless. Patients and clinicians often lack a shared understanding of a patient’s goals 13 . Patients struggle to get the information they need to transition home from hospitals, understand care instructions, and get information about post-care symptoms and complications 7 . People with chronic illnesses struggle to monitor information about their illness and share it with providers 18 . The problem of coordinating care across multiple providers, a patient, and their community is fundamentally an information systems problem, and one poorly supported by technology, health care communication practices, and the varying complexity of health care funding in different countries. The result is that many patients take care into their own hands, using self-tracking technology such as consumer devices like fitness trackers 5 , and even hacking their own monitors. The result is often an even more complex challenge of integrating the data that people have gathered about themselves with the existing information systems of their health care providers 12 .
The provider side of health care from inside these information systems is similarly complex. Providers and hospitals often have few ways to overcome the poor design and usability of electronic medical records other than simply hiring more staff to workaround these problems 16 . Medical records often fail to capture emotional information in facial expressions and voice, crucial to critical care and emergency room practice 11 . And at the heart of many of these challenges are the new and underlying information technology challenges that store, retrieve, and secure medical data, creating issues of poor data interoperabilityinteroperability: The ability to move and translate data structures between different systems without losing data or changing its meaning. between health care silos, complexities of regulatory compliance with privacy policy like HIPPA, and the regular disruptions of IT in general, such as confusing software updates, internet outages, and hardware failures 8 . Many of these problems emerge from the fragmentation of decentralized health systems; countries that invested in universal health care systems post World War II benefit from much more uniform, centralized systems, simplifying improvements and eliminating many interoperability problems.
Atop all of these challenges with individual patients are population health challenges 9 , which consider entire communities of people and their health. Population health includes disciplines like epidemiology, which gathers, analyzes, and reports data about both determinants of health, as well as diseases, through populations. This includes people charged with detecting and preventing the spread of deadly bacteria and viruses, as well as people monitoring the use of substances like nicotine and other controlled substances. Complementing epidemiology is public health , which is more concerned with proactively preventing disease and promoting wellness. This discipline focuses on disseminating information, including providing health education to prevent deterioration of health. For example, public health practitioners lead efforts on safe sex campaigns, needle-exchange programs to prevent the spread of communicable diseases through reused needles, and advocating for smoking cessation. At the heart of both of these disciplines are questions of health equity, which recognize that in many societies, only some people have the resources they need to stay healthy and well. This increasingly includes information and technology resources, such as access to the internet and health information technologies, like blood sugar monitors for patients with diabetes.

At the foundation of all of these intersections between information and health are issues of diversity, equity, and inclusion. Biology is inherently diverse, human experiences are inevitably diverse, and yet so much of our understanding of DNA, effective medicine, and population health stems from studies that often systematically exclude significant parts of that diversity, or erase it through aggregate statistics. These practices of supporting health through a lens of dominant groups results in systemic inequality in who is treated, who is treated effectively, and therefore who lives long, healthy lives. Challenges in information and health, therefore, are fundamentally health equity challenges 4 , and how we gather, store, and use information about our health is at the center of how we ensure equity.
Podcasts
For more about the intersection of health and information, consider these podcasts:
- The Ashes on the Lawn, Radiolab . Describes the history of HIV/AIDS advocacy, and the response of the U.S. federal government to this advocacy.
- The Great Vaccinator, Radiolab . Describes the contributions of Maurice Hilleman, inventor of more than 40 vaccines, many routinely given to children.
- The Science Behind The Historic mRNA Vaccine, Short Wave . Describes the science behind the mRNA technology used in the Pfizer-BioNTech COVID-19 vaccine.
- Down and Dirty with Covid Genes, In Machines We Trust, MIT Technology Review . Describes the many ways that DNA scrubbing and machine learning is being used to detect and treat disease.
- The Rise of Therapy Apps, What Next TBD, Slate . Discusses a new genre of therapy apps intended to scale access to mental health, as well as their limitations, and the risks of lowering the bar on care.
- How AI is giving a woman back her voice, In Machines We Trust . Discusses applications of voice recognition in health care.
- What Does It Mean to Give Away Our DNA?, The Experiment . Discusses the tensions between genetic testing and Indigenous communities.
- The Downfall of One of the World’s Biggest Brains, What Next TBD . Discusses IBM Watson’s failulre to transform health care.
References
-
Andreas D. Baxevanis, Gary D. Bader, David S. Wishart (2020). Bioinformatics. John Wiley & Sons.
-
Arun Bhatt (2010). Evolution of clinical research: a history before and beyond James Lind. Perspectives in Clinical Research.
-
Allan M. Brandt (1978). Racism and research: the case of the Tuskegee Syphilis Study. Hastings Center Report.
-
Paula Braveman (2006). Health disparities and health equity: concepts and measurement. Annual Review of Public Health.
-
Daniel A. Epstein, Monica Caraway, Chuck Johnston, An Ping, James Fogarty, and Sean A. Munson (2016). Beyond abandonment to next steps: understanding and designing for life after personal informatics tool use. ACM Conference on Human Factors in Computing Systems.
-
Vicki S. Freimuth, Sandra Crouse Quinn, Stephen B. Thomas, Galen Cole, Eric Zook, and Ted Duncan (2001). African Americans’ views on research and the Tuskegee Syphilis Study. Social Science & Medicine.
-
Shefali Haldar, Sonali R. Mishra, Maher Khelifi, Ari H. Pollack, and Wanda Pratt (2019). Beyond the Patient Portal: Supporting Needs of Hospitalized Patients. ACM Conference on Human Factors in Computing Systems.
-
William Hersh (2004). Health care information technology: progress and barriers. Journal of the American Medical Association.
-
David Kindig and Greg Stoddart (2011). What is population health?. American Journal of Public Health.
-
Michael Marmot, Richard Wilkinson (2005). Social determinants of health. OUP Oxford.
-
Helena M. Mentis, Madhu Reddy, and Mary Beth Rosson (2010). Invisible emotion: information and interaction in an emergency room. ACM Conference on Computer Supported Cooperative Work and Social Computing.
-
Helena M. Mentis, Anita Komlodi, Katrina Schrader, Michael Phipps, Ann Gruber-Baldini, Karen Yarbrough, and Lisa Shulman (2017). Crafting a View of Self-Tracking Data in the Clinical Visit. ACM Conference on Human Factors in Computing Systems.
-
Ari H. Pollack, Sonali R. Mishra, Calvin Apodaca, Maher Khelifi, Shefali Haldar, and Wanda Pratt (2020). Different roles with different goals: Designing to support shared situational awareness between patients and clinicians in the hospital. Journal of the American Medical Informatics Association.
-
Leslie A. Pray (2008). Discovery of DNA structure and function: Watson and Crick. Nature Education.
-
Wynand P. Roos, and Bernd Kaina (2006). DNA damage-induced cell death by apoptosis. Trends in molecular medicine.
-
Gordon D. Schiff, and Laura Zucker (2016). Medical scribes: salvation for primary care or workaround for poor EMR usability?. Journal of General Internal Medicine.
-
Kendra L. Schwartz, Thomas Roe, Justin Northrup, James Meza, Raouf Seifeldin, and Anne Victoria Neale (2006). Family medicine patients’ use of the Internet for health information: a MetroNet study. The Journal of the American Board of Family Medicine.
-
Lisa M. Vizer, Jordan Eschler, Bon Mi Koo, James Ralston, Wanda Pratt, and Sean Munson (2019). “It’s Not Just Technology, It’s People”: Constructing a Conceptual Model of Shared Health Informatics for Tracking in Chronic Illness Management. Journal of Medical Internet Research.
-
Duojiao Wu, Catherine M. Rice, and Xiangdong Wang (2012). Cancer bioinformatics: A new approach to systems clinical medicine. BMC Bioinformatics.