| Alzheimer's Disease |  |
| Alzheimer's Disease | |
What is Alzheimer's Disease?In 1986, President Ronald Reagan's "I don't remember," "I don't recall" responses seemed to many to be lame answers to questions about political dealings. However, it turns out that they may have been the truth. In 1994, former President Ronald Reagan announced that he had Alzheimer's disease (AD). |  Ronald Reagan |
 |
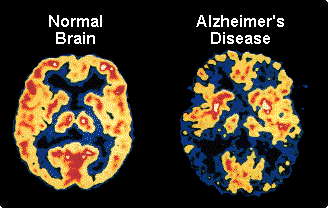
Alzheimer's disease attacks the brain; it is not a normal part of aging. People with AD have a gradual memory loss and difficulties with language and emotions. The progressive loss of intellectual abilities is termed dementia. As the disease advances, the person may need help in all aspects of life: bathing, eating, and using the restroom. Because of this round-the-clock care, families and friends of people with AD are greatly affected. The disease is irreversible and there is currently no cure. |
Who Gets AD?About 5-6% of the US population has AD or a related dementia. This means that approximately four million Americans have AD. As the population ages, the burden to caregivers and cost to society will grow. It is estimated that by 2050, 14 million people in the US will suffer from AD.Alzheimer's disease ranks fourth in the cause of death among adults. About 100,000 people die per year as a result of AD. Five to 10 percent of the population over age 65 have AD. At the age of 85 and older, about 50% have AD. Although age is a factor, research has shown that genetics also play a role. Because women tend to live longer than men, more women are affected by AD than men. Furthermore, 80% of caregivers are women, so they are also secondarily affected by the disease. | Estimated Number of Cases of AD in the U.S. (millions)  |
 |
SymptomsMemory loss, especially of recent events and newly acquired information, is perhaps the most noticeable trait of AD. The first symptoms have a gradual, subtle onset, and can be a sign of many dementias, not just AD. For example, a person may become lost in familiar surroundings, forget whether a task was done, repeat the same story, or is unable to learn new things. As the disease worsens, the person may be unable to find the right word or to make responsible decisions. |
|
One of the most painful aspects of the disease is that the person
sometimes will not recognize friends or family members. Personality
changes can occur, such as unusual agitation, paranoia, depression, and
social withdrawal. Later, people with AD may wander, or be unable to find
their way home. New research, however, has shown that a part of the brain
that processes visual and spatial information may be damaged in people
with AD. This may account for the problems AD patients have with
orienting themselves.) Patients may also become inattentive, thus unable
to care for their day-to-day bodily needs. Other parts of the brain
including the basal forebrain and hippocampus, areas important for memory,
are also affected by AD. Many AD sufferers die from other causes such as
pneumonia. From the time of diagnosis, AD patients generally live 6-8
years, although many live for as long as 20 year after the diagnosis. The symptoms of AD vary tremendously from person to person, but in time, each person who has AD will experience worsening symptoms. Many of the behavioral changes associated with AD - depression, paranoia, and delusions - can be helped with medication. However, there is no cure for AD, although some treatments hold promise. | Areas of
the brain affected by AD 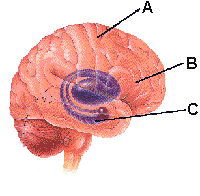 A = Cerebral Cortex B = Basal Forebrain C = Hippocampus Image courtesy of the NIA |
A Closer Look at an AD BrainThe microscopic changes that occur in the brain of a person with AD were first noted by German neurologist Alois Alzheimer in 1906. He performed an autopsy on a woman who had become more and more confused in the years preceding her death. He called the changes he observed in her brain plaques and tangles. These features can only be seen upon autopsy. Tangles and plaques interfere with neuronal functions, such as communicating with each other and sending messages to other parts of the body.Research suggests that the formation of tangles in the brain may be a part of the normal aging process. Dr. John Morris of Washington University School of Medicine in St. Louis, Missouri, published a report titled "Tangles and plaques in nondemented aging and preclinical Alzheimer's disease" in the March 1999 issue of Annals of Neurology, Volume 45 Number 3, pages 358-368. This study showed that of the 39 nondemented people (people with no behavioral evidence of Alzheimer's disease), all had tangles in their brains. So perhaps developing tangles is an inevitable part of growing old. "This is further evidence that there is such a thing as truly healthy aging and that Alzheimer's disease is not inevitable," states Morris. More research is needed to figure out what role tangles and plaques play in AD. Are only plaques responsible, or do tangles and plaques interact? Other observed changes in the brain affected by AD include:
|
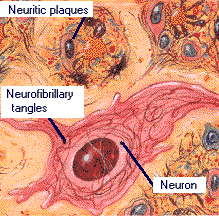
Image courtesy of the NIA |
Neurofibrillary TanglesIt is unclear how neurofibrillary tangles (NFT) form. NFTs are found inside of the neuron: the neurons themselves become deformed and clump together. NFTs have been described as looking like a rope tied in knots. A protein named tau has been shown to be involved in forming NFTs, but more research is needed to solve the mystery of how and why NFTs form, and how exactly they affect the brain.
PlaquesUnlike tangles, plaques occur outside the neuron. Plaques are mainly composed of a protein called beta amyloid, although other proteins contribute to plaque formation. Research has shown that a protein in our bodies called amyloid plays a significant role in AD. Proteins are vital molecules that control all sorts of processes in our body. The amyloid protein occurs naturally in our brains, but as we age, too much of it (in a form called beta amyloid) accumulates in the brain, forming plaques. Beta amyloid is formed when an enzyme clips the amyloid precursor protein; beta amyloid, a fragment from this process then aggregates in deposits. It is unknown whether these deposits are due to excess production or whether the enzymes that usually break it down are not functioning properly. This situation is similar that of cholesterol in our bodies. Some cholesterol is needed to keep our cells healthy, but too much cholesterol can block arteries and lead to heart attacks and other problems. |
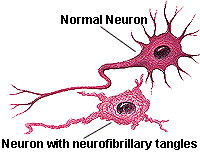 Image courtesy of the NIA Illustrator: Lydia Kibiuk |
Drug Therapies Four drugs for treating AD have been approved by the US Food and Drug
Administration (FDA): Donepezil
(Aricept), rivastigmine
(Exelon) and galantamine
(Razadyne) are used to treat mild to moderate Alzheimer's disease and
memantine
(Namenda), is used to treat moderate to severe Alzheimer's.
Doneprezil, rivastigmine and galantamine are drugs classified as
cholinesterase inhibitors. These drugs inhibit the breakdown of
acetylcholine by blocking the action of cholinesterase, the key enzyme in
the breakdown of acetylcholine. Both drugs increase the level of the
acetylcholine in the brain. These drugs also slow memory loss and help the
person perform daily tasks. Memantine is a NMDA receptor antagonists that
decreases abnormal activity in the brain. This drug can help people think
and remember. It is important to note that all of these drugs are not a
cure, they only lessen the symptoms of AD.
Four drugs for treating AD have been approved by the US Food and Drug
Administration (FDA): Donepezil
(Aricept), rivastigmine
(Exelon) and galantamine
(Razadyne) are used to treat mild to moderate Alzheimer's disease and
memantine
(Namenda), is used to treat moderate to severe Alzheimer's.
Doneprezil, rivastigmine and galantamine are drugs classified as
cholinesterase inhibitors. These drugs inhibit the breakdown of
acetylcholine by blocking the action of cholinesterase, the key enzyme in
the breakdown of acetylcholine. Both drugs increase the level of the
acetylcholine in the brain. These drugs also slow memory loss and help the
person perform daily tasks. Memantine is a NMDA receptor antagonists that
decreases abnormal activity in the brain. This drug can help people think
and remember. It is important to note that all of these drugs are not a
cure, they only lessen the symptoms of AD. Many other drugs for treating AD are awaiting approval from the US FDA.
Other Therapies
|
Expanding Diagnostic ToolsBecause a definitive diagnosis of AD can only be made by examining the brain after a person dies, AD diagnosis in the living must be made by exclusion. This means that other diseases must be ruled out as a cause of the dementia. There is no single test to show that a person has AD, but several tests can suggest the presence of AD.
 |
Risk FactorsFirst and foremost, the chance of developing AD increases with age. With each additional year of life, there is increased likelihood that one will display symptoms of AD. Alzheimer's disease affects men and women about equally, and strikes all ethnic groups.There are actually two types of AD: familial (early onset) and sporadic (late onset). Familial AD is a rare form of AD that affects a small subset of people at a younger age, usually before their fifties. It has a strong genetic component: mutations on genes 21, 14, and 1 cause a predisposition to AD.(Reported in Neurology, July 1998.) Sporadic (late-onset) AD is the type most people are familiar with. It affects people most often after they reach 65 years of age. A gene called ApoE on chromosome 19 has been pinpointed as being a risk factor for AD. |
What Can You Do to Protect Your Brain As You Age?As you age, some connections in your brain may fail due to tangles or plaques, so it makes sense that the more neural connections you have overall, the more you will be able to compensate for the damaged connections. It's like a sports team. If one player gets injured and there is a qualified player on the bench who can substitute, the team will still function well. The more players available to play for injured team members, the better the team will fare.How do you get and maintain neural connections? It is thought that staying active, both mentally and physically, will help. Challenge your mind. Remember people's names. Work crossword puzzles. Do math. Read. Learn new words. |
 |
Future ResearchUnderstanding Alzheimer's disease is one of the most active areas in neuroscience research. In 1998, scientists took a big step forward by breeding mice that develop the symptoms of AD. These mice will help researchers unravel the mysteries of AD. Research into future treatments can be divided into several categories.
Chemical Theories
The Genetic TheoryThe genetics of AD are confusing at best. Some families may have many members affected, but because family members may be exposed to the same environment, it is impossible to say how much heredity is to blame. Several genes have been identified on chromosomes 21 and 14 in the familial type of AD. In the more common sporadic type, people with a gene for a protein called apolipoprotein E on chromosome 19 tend to have a higher incidence of AD than the general population. Much more work needs to be done to fully understand how genetics influences the incidence of AD.
The Autoimmune TheoryYour immune system fights off infection from bacteria, viruses, and other threats to your well-being. If this system goes awry, your immune system can attack its own tissue. Scientists hypothesize that if your immune system attacks your brain as you age, AD symptoms could result. However, it is unclear whether this leads to AD, because signs of this type of attack have been seen in non-AD brains.
The Slow Virus TheorySome brain disorders which cause symptoms similar to AD are caused by slow viruses. However, no one has identified a virus specific for AD. |  |
They said it! | "Alzheimer's can be called the long
goodbye. You grieve about the loved one from the moment you begin
to observe the gradual loss of memory and the speech and personality
changes, because they are incurable. The person you love is
gradually changing before your eyes. You say good-bye many times
until the final good-bye at death." --- Norma Wylie, 1996 (in Sharing the Final Journey: Walking with the Dying)
|
References and further information
|
| BACK TO: | Exploring the Nervous System | Table of Contents |
![[email]](./gif/menue.gif) Send E-mail |
![[newsletter]](./gif/menunew.gif) Get Newsletter |
![[search]](./gif/menusea.gif) Search Pages |
 Donate to Neuroscience for Kids |
This article prepared by Ellen Kuwana
Neuroscience for Kids Staff Writer
Last revision: March 25, 2020.