Welcome to The UW Shoulder Site @ uwshoulder.com

Please note that information on this site was NOT authored by Dr. Frederic A Matsen III and has not been proofread or intended for general public use. Information was intended for internal use only and is a compilation for random notes and resources.
If you are looking for medical information about the treatment of shoulders, please visit shoulderarthritis.blogspot.com for an index of the many blog entries by Dr. Frederick A Matsen III.
Da Book
Standard Operating Procedures and Notes for the Shoulder Team
Ordering X-Rays in Clinic
X-rays and other imaging are one of the big four in diagnosing shoulder and elbow problems (the four being- Hx, SST, PE, and X-ray/films).
All patients need to have a current x-ray for evaluation purposes. Patients with MRIs only, outside films and out dated x-rays taken here (more than 6 months) - need new films done by our techs. All new patients must have an x-ray.
MAs and Nursing Staff - Please have all females remove their bras and put on a gown prior to calling x-ray to get the patient. Bras often have metal in them that show up in the shoulder field and cause delays as patients must be refilmed.
Centricity
Residents, students and staff on the Shoulder and Elbow Service need to have a PACs account and be familiar with using Centricity.
Centricity Quick Reference Guide
If you need a PACS account created, phone the UWMITS Helpdesk at: (206) 543-7012
or
Send an email to:
mcsos@u.washington.edu and give them the following information:
Full Name:
AMC/Mindscape Login Name:
Position Title:
Department:
Physician ID or Staff ID:
Contact Number and Email address:
Access needed (HMC, UW, or both):
X-Rays by Complaint
Arthritis Rotator Cuff Tear (first visit only)
Shoulder Pain
Arthritis series (Axillary, Grashey, and Template of Shoulder)
Clear History of: Instability
Bankart lesion
Hx of dislocation
"shoulder keeps coming out of joint"
If not clear - Arthritis Series
Instability Series Anything about elbow 4 view Elbow True fracture of Humerus AP and Lat of Humerus AC separation AC Series Bilat with and without weights SC separation Serendipity View AP SC Joint
When in doubt Arthritis series (Axillary, Grashey, and Template of Shoulder)
X-Rays by Series
Arthritis series
Most patients need a three view arthritis series (Axillary, Grashey, and Template of Shoulder).
Indication: Arthritis, Rotator Cuff Tear (first visit only), Pain
Instability Series
If patients are complaining about instability, you can order an instability series. This can be confusing since many patients are not sure how to describe their shoulder symptoms and often say they are unstable due to arthritis or pain. Unless it is clear that they are unstable or had a dislocation, go ahead and order an arthritis series.
Indication: Instability, Bankart lesion, Hx of dislocation, "shoulder keeps coming out of joint"
4 view Elbow
Elbow complaints need a 4 view of the elbow
Indication: Anything about elbow
AP and Lat of Humerus
Fractured humeri need an AP and Lateral of Humerus
Indication: True fracture of Humerus
AC Series Bilat with and without weights
This is for AC separations.
Indication: AC separation
Serendipity View
If a patient has pain or instability in sternum area they need an Serendipity View of the SC joint. You may also need to do an AC series to assess the Clavicle.
Indications: SC separation
When in doubt - order an arthritis series.
The Views
Grashey AP
Done properly, this view should line up the glenoid so that it is perpendicular with the plane of the xray. This allows for better evaluation of gleneral-humeral joint space, and position of the humeral head in relation to the glenoid. With the humerus adducted, you can better assess if there may be humeral bone contacting the inferior glenoid - what is often referred to as "Poo Corner."
The UW Radiology site has an excellent example of this view.
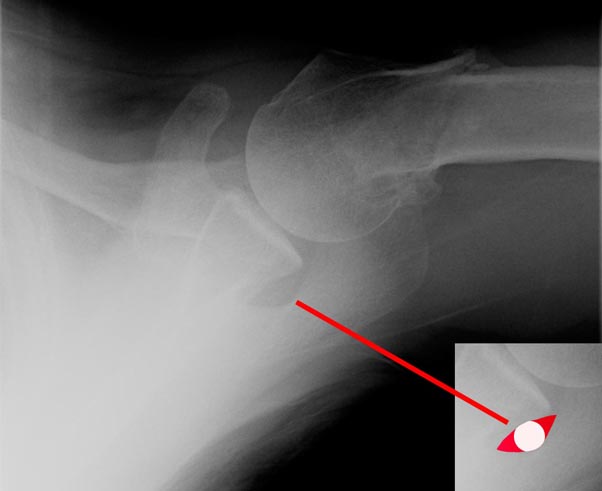
True Axillary
Done properly, this view allows of assessment of humeral wear in the anterior and posterior planes. And if aligned just right, it should show bone defects in the anterior glenoid lip.
This view is actually difficult to get just right, even by a skilled radiology tech. A true axillary view will have an "eye" just posterior to the glenoid (see image above). If this eye is not present, the anterior glenoid edge will be obliqued by the superior or inferior glenoid edge - which may mask severe defects that only a properly aligned axillary view will reveal. If the "eye" is not seen on the axillary view, this shot should be redone.
This view may also show decreased joint space, fractures, osteophytes, dislocations, Hill Sachs and reverse Hill Sachs Lesions.
The UW Radiology site has an excellent example of this view.
Stryker Notch View
The patient is supine on the table with the cassette placed under the shoulder. The palm of the hand of the affected shoulder is placed on top of the head, with the fingers directed toward the back of the head. The elbow of the affected shoulder should point straight upward. The x-ray beam tilts 10° toward the head, centered over the coracoid process (see se above).
The goal of this view it to catch a humeral head defect in patients with a history of recurring anterior dislocation of the shoulder.
Apical Oblique View
In this technique the patient sits with the scapula flat against the cassette (as for the AP view in the plane of the scapula). The x-ray beam is centered on the coracoid and directed perpendicular to the cassette (45° to the coronal plane) except that it is angled 45° caudally. The beam passes tangential to the articular surface of the glenohumeral joint and the posterolateral aspect of the humeral head.
This view is likely to reveal both anterior glenoid lip defects and posterior lateral impression fractures of the humeral head.
Shoulder AP with Internal Rotation
The UW Radiology site has an excellent example of this view.