Methods
Subjects
Seven individuals with OA of the medial knee who ambulate with a walking cane were recruited from the Veteran’s Affairs Puget Sound Healthcare System (VAPSHCS). The participants qualified for the study by having radiographic evidence of medial tibiofemoral knee osteoarthritis, were aged 35 years or older, had the ability to stand with periodic bouts of walking for at least 30 minutes without difficulty, and used a walking cane. The exclusion criteria included prior knee joint replacement or recent (<1 year) surgical, neurological, rheumatologic or other musculoskeletal problem that might impair the measures in the study, inadequate cognitive or language function to consent or to participate, body weight greater than 300 lbs, and being pregnant. This study was approved by the VAPSHCS IRB. All participants provided written consent.
Gait Lab Data Collection
Prior to data collection each participant was asked to complete the Western Ontario and McMaster Universities Osteoarthritis Index (45L) to assess the pain, stiffness, and physical function of their knee joint. Anthropometric and demographic data were collected in addition to a short medical history regarding their knee OA. Following data collection, the participants were asked to complete a survey on their thoughts and attitudes towards the smart cane.
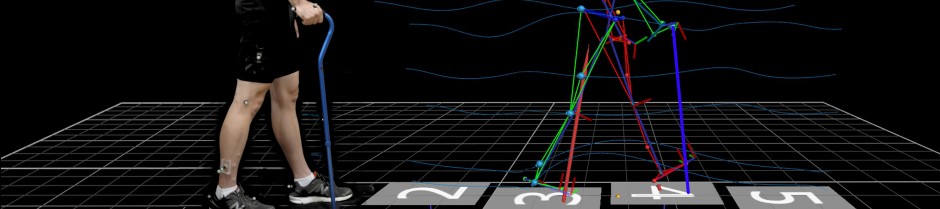
The study subjects underwent three-dimensional gait analysis in a single session that involved a static trial and four walking conditions. Trials from each condition were recorded using a 12 camera Vicon (Lake Forest, CA) motion analysis system. In addition, trials were performed over force plates (AMTI, Watertown, MA) placed in the laboratory floor in order to measure the ground reaction forces of the gait cycle and recorded the kinematics and kinetics of each subject at 120 Hz and 1200 Hz, respectively. Thirty-five reflective markers were placed over anatomical landmarks on the upper and lower limbs, trunk, and head in order to establish joint centers according to the Vicon Plug-In-Gait full-body model. In addition, five markers were placed on the cane in order to establish its position during motion analysis.
The smart cane was a standard aluminum cane fitted with a load cell near the base of the cane, data collection hardware within the shaft, and batteries and a vibrating motor in the handle. The cane measured longitudinal forces through the cane at 100 Hz and stored the cane loading peaks of each step. This data was compared to force plate data as a gold standard. The cane was adjusted to the distal wrist crease as established by Kumar et al. (72L) prior to collection of data and synchronized with the Vicon motion capture system via a wired trigger.
Participants were asked to walk a 19.63 m hallway using their own cane to determine their self-selected walking speed. Walking trials were completed within 10% of each subject’s self-selected speed. Following the collection of the self-selected walking speed, reflective markers were placed on the participants and a static trial was conducted to identify joint centers. Afterwards, participants completed four dynamic walking conditions. Each condition was performed until five satisfactory trials were logged. The participant needed to make 2-3 consecutive force plate strikes and be within 10% of their self-selected walking speed for a trial to be logged. Gait speed was measured by photoelectric timing gates placed 2 meters apart. The participants were kept naive of the purpose of the force plates so as not to alter their gait in an effort to make consecutive strikes. The four conditions included: unaided walking, naive cane use, cane use with three-point gait instruction and demonstration of how 20% body weight loading of the cane felt by using a scale, and smart cane use with vibrotactile biofeedback when at least 20% of their body weight was placed through the cane. Both the instructed and smart cane condition were divided into two five trials sessions that were separated by a five minute rest. This was done to allow the retentive abilities of both trainings to be studied. Scale training was selected to represent a currently available PWB teaching method and compare it to the teaching ability of the smart cane. 20% body weight was selected based on Simic et al’s finding that cane loading at that body weight was as or more effective at reducing KAM than other conservative treatments such as lateral wedge orthoses and knee braces (40L). The smart cane was used for all conditions in which a cane was required and its force-measuring abilities were activated for each condition, but the vibrating motor was only active during condition four. Normalized verbal instructions were given before the start of each condition. Instructions to use the cane contralateral to the affected knee (73L,75L) and advance it simultaneously with the opposite leg to permit the heel and cane contact the ground at the same time were given prior to condition three and four. The subjects were allowed to practice prior to the data collection of each condition in order to familiarize themselves with the expectations.
The order of the conditions was standard for the first two while the final two were randomized. The first condition established baseline gait forces when the subject is unaided by a cane. Condition two represented the typical cane force used by the subject. The third condition illustrated the participant’s ability to place 20% body weight through the cane after verbal instruction of the current standard of care for cane use and an ability to learn to load the cane to 20% using a scale. Condition four established the subject’s ability to apply 20% body weight with the assistance of vibrotactile biofeedback.
Downloadable Resources
- Data Collection and Processing Protocol For Smart Cane
- Visual 3D Pipeline Filter and Gait Events
- Visual 3D Pipeline Angle Moment Power Left
- Visual 3D Pipeline Angle Moment Power Right
- Visual 3D Pipeline Export Stance Left
- Visual 3D Pipeline Export Stance Right