
New Stroke Protocol Imaging algorithm:
- Stroke Code patient comes to CT
- Non-contrast Head CT done first
- If blood in head, then CTA Head, then done
- If no blood in head, then CTA Neck
- CTA neck will be read in (near) real time by NeuroRads/Rads Att/Fellow if available, or at least Rads R4 resident (optimally with Neurology resident at shoulder also reading)
- If anterior LVO (defined as any of ICA occlusion (cervical or intracranial), M1 occlusion, M2 occlusion), then order and perform CTP
- If there is any debate about anterior LVO delaying patient in scanner, default to DO CTP
- If basilar artery thrombosis, then Code Stroke MRI. Portable CXR and KUB to be obtained in the CT suite for MR clearance.
Thus, the major change is that CTP is only to be done on patients with documented LVO, as opposed to current system where it is being done for all ischemic stroke codes. Hopefully this will improve efficiency for all.
For the graphically oriented:
Dr. David Terschwell
Effective December 1, 2017
Updated by JDR 2/16/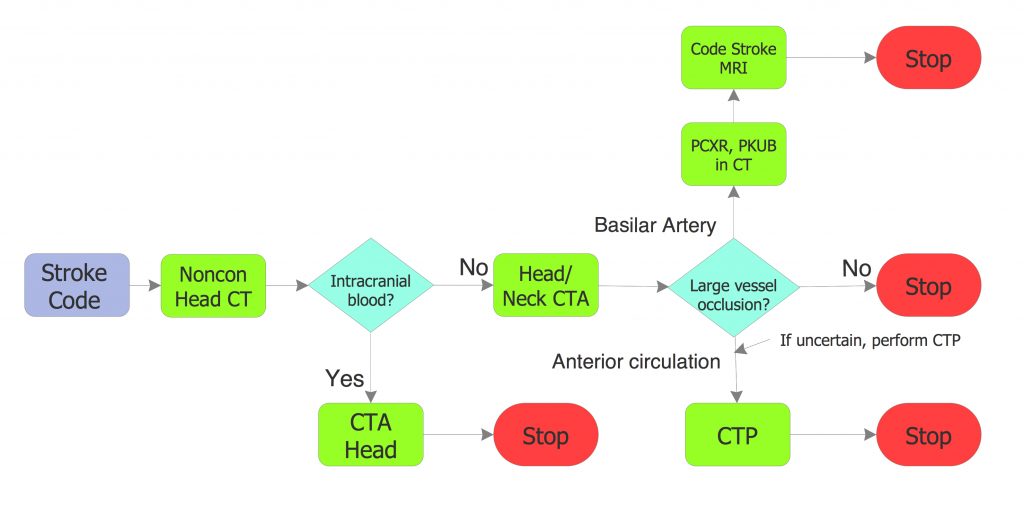 2018
2018