Dream Interpretation and False Beliefs
Giuliana A. L. Mazzoni
University of Florence
Pasquale Lombardo
University of Bolgna
Stefano Malvagia
University of Florence
Elizabeth F. Loftus
University of Washington
ABSTRACT
Dream interpretation is a common practice in psychotherapy. In the research
presented in this article, each participant saw a clinician who interpreted a
recent dream report to be a sign that the participant had had a mildly
traumatic experience before age 3 years, such as being lost for an extended
time or feeling abandoned by his or her parents. This dream intervention
caused a majority of participants to become more confident that they had had
such an experience, even though they had previously denied it. These findings
have implications for the use of dream material in clinical settings. In
particular, the findings point to the possibility that dream interpretation
may have unexpected side effects if it leads to beliefs about the past that
may, in fact, be false.
Part of this study was supported by a MURST Grant.
Correspondence may be addressed to Giuliana A. L. Mazzoni, Department of
Psychology, University of Florence, via S Niccolo'89/a, Florence, Italy, 50125.
Received: July 25, 1997
Revised: April 3, 1998
Accepted: April 20, 1998
Dream interpretation is a common current clinical tool used more in some
therapies than in others ( Brenneis, 1997 ). Although this
tool might not necessarily be problematic as an enterprise, what would be the
impact and consequence of a clinician imposing an incorrect interpretation on
dream material? Could sbuch misinterpretation influence patients' beliefs about
their past in ways that might be detrimental? Could patients be led to false
beliefs about their past?
Dream material was viewed by Sigmund Freud (1900/1953 , 1918/1955
) as providing a royal road to the unconscious and as being a vehicle for
unearthing specific traumatic experiences from the past. Psychoanalytic theory
and technique (including dream interpretation) dominated psychotherapy training
well into the 1950s, when behavioral, humanistic, and cognitive approaches,
which do not emphasize dream interpretation, began to have greater impact. Dream
interpretation, or dream work, holds a far less central position among clinical
intervention tools than it did just 30 years ago.
Nonetheless, a sizable percentage of professional psychologists today report
using dream interpretation in their clinical work ( Brenneis, 1997
; Polusny & Follette, 1996 ; Poole,
Lindsay, Memon, & Bull, 1995 ). Moreover, a subset of clinicians who
work in the area of trauma view dreams being "exact replicas" of the
traumatic experiences ( van der Kolk, Britz, Burr, Sherry, &
Hartmann, 1984 , p. 188). For example, one therapist wrote, "Buried
memories of abuse intrude into your consciousness through dreams ... Dreams are
often the first sign of emerging memories" ( Fredrickson,
1992 , p. 44). Another therapist wrote,
Repressed memory dreams are dreams that contain a partial repressed memory or
symbols that provide access to a repressed memory. During sleep, you have a
direct link to your unconscious. Because the channel is open, memory fragments
or symbols from repressed sexual abuse memories often intrude into the dream
state. Even though the memory is embedded in the symbolism of the dream world,
it is possible to use the dream to retrieve the memory. ( Fredrickson,
1992 , p. 125)
Does this sort of clinical dream interpretation actually lead to the recovery
of a genuine traumatic past? Or is it possible that the dream interpretation
might be leading people to develop false beliefs, or even false memories, about
their past? And if so, is it harmful?
We recently published several studies that may have some relevance to these
questions ( Mazzoni & Loftus, 1996 ). We showed that after
a single subtle suggestion, participants falsely recognized items from their
dreams and thought that these items had been presented in a list that they
learned during the waking state. Our participants first learned a key list of
words. In a later session, they received a false suggestion that some items from
their previously reported dreams had been presented on the key list. Finally, in
a third session, they tried to recall the items that had occurred on the initial
key list. A major finding was that participants often falsely recognized their
dream items and thought they had been presented on the key list, sometimes as
often as they accurately recognized true list items. Despite the high rate of
false recognition, and the conviction that participants had about these false
memories, it is reasonable to question whether the same kind of results would
occur with more personally meaningful events.
The Florence False Interpretation Study
We devised a new methodology for exploring whether such activities can lead
people to develop false beliefs about the past. We found individuals who
reported that it was unlikely that they had had certain critical experiences
before the age of 3 years. The age of 3 years is important to shed light on
whether changes that resulted from our manipulation were due to the recovery of
true experiences or the creation of false ones ( Wetzler
& Sweeney, 1986 ). The critical experiences included episodes like being
lost in a public place for some extended time. Later, some of these individuals
went through a 30-min minitherapy simulation with a clinical psychologist, who
interpreted their dream (no matter what the content of the dream) as if it were
indicative of having undergone specific critical experiences in the past.
An initial group of 128 undergraduates from the University of Florence filled
out an instrument that we called the Life Events Inventory (LEI) on which they
reported on the likelihood of various childhood events having happened to them.
The LEI has 36 items, 3 of which are critical items. The inventory asks
participants to consider how certain (confident) they are that each event did or
did not happen to them before the age of 3 years. Participants respond by
ranking items on an 8-point Likert-type scale ranging from 1 ( certain it did
not happen ) to 8 ( certain it did happen ). Fifty participants who
had low scores (below 4) on the 3 critical items were selected and asked to
participate in the next phase of the study. The 3 critical items were as
follows: "got lost in a public space," "was abandoned by my
parents," and "found myself lonely and lost in an unfamiliar
place." The cover story associated with the administration of the LEI
explained that the study concerned the frequency of rare and common events that
happened during early childhood and that the study goal was the validation of an
instrument to measure these experiences.
Of the selected 50 participants, half were randomly assigned to a dream
condition, where they received suggestive information about the content of their
dream. The other half did not receive any suggestive information about their
dreams. Of the 25 participants in the dream condition, only 19 completed all
three phases of the experiment; all 25 participants in the non-dream condition
completed the experiment. (The difference in completion rate appeared to be due
to a handful of participants who were randomly assigned to the dream condition
but chose not to participate in what they thought was an additional experiment.
Whether this choice was due to already having sufficient credits or some other
reason was not explored.) The mean age of the final sample of 44 participants
was 21 years, and 64% were women.
All 44 participants returned to take the LEI again after 3 to 4 weeks.
However, those in the dream condition also participated during that time in what
they thought was a completely different experiment but was actually the dream
manipulation.
For the participants in the dream condition, dream interpretation was done
10-15 days after the first LEI. Shortly before the dream session, dream
condition participants received a phone call from a clinician asking for their
participation in a dream and sleep study. Participants were asked to bring in
one or more dreams, which could be a recurrent dream, a recent dream, or a vivid
dream (no constraints were put on the type of dream). These participants had
their dreams individually interpreted by a clinical psychologist. The particular
clinician is a trained clinical psychologist with a private practice in
Florence, Italy. He also is well known in the community from his radio program
on which he gives clinical advice. Moreover, he has a strong, persuasive
personality. In the dream session, the clinician welcomed the participants and
explained that the purpose of the study was to collect meaningful dreams and to
relate those dreams to sleep characteristics. Then the participants read their
own dream report aloud. Next, the clinician asked participants for their own
interpretation of the dream and for their comments on the dream. Then the
clinician offered his own comments. The comments were framed in terms of a
clinical interview (i.e., the psychologist followed a predefined script but was
free to make some modifications depending on the responses of the participant).
Early on, he explained that he had considerable experience in dream
interpretation, and he explained that dreams are meaningful and symbolic
expressions of human concern.
A key feature of the dream manipulation was to suggest to participants that
the dream was the overt manifestation of repressed memories of events that
happened before the age of 3 years. To be specific, the dream interpretation
suggested to the participants that the dream was indicative of a difficult
childhood experience, such as getting lost in a public place, being abandoned by
one's parents, or being lonely and lost in an unfamiliar place-the three
critical items. No matter what the content of their dreams, all participants
received the same suggestion: that one or more of these critical experiences
appeared to have happened to them before the age of 3 years.
To appreciate what the clinician did with the specific dream material, it is
helpful to use a concrete example. Suppose a participant came in with a dream
report about walking up a mountainside alone on a chilly day and commented that
the dream must mean that he finds mountain walking appealing. The clinician
might then discuss part of the dream, mentioning the mountain, that the
participant reported being alone there, and that despite the participant's
remark about liking mountain walking, the "chilly day" suggests that
the experience might be a "cold" one for the participant. At that
point, the clinician would try to induce the participant to agree with this
suggestion. The clinician might then move toward a global interpretation,
suggesting that in his vast experience with dream interpretation, a dream like
this usually means that the participant is not totally happy with himself, he
needs challenge, he resists being helped by others, and he might have social or
interpersonal difficulties. The clinician then might suggest to the participant
that the dream content, and the feelings about that dream, are probably due to
some past experience that the participant might not even remember. The clinician
would then tell the participant that the specific details mentioned are commonly
due to having had certain experiences before age 3, like being lost in a public
place, being abandoned even temporarily by parents, or finding oneself lonely
and lost in an unfamiliar place. Finally, the clinician would ask whether any of
the critical events happened to the participant before the age of 3 years. When
the participant claimed not to remember these experiences, the clinician
explained how childhood experiences are often buried in the unconscious but do
get revealed in dreams.
From this example, it is easy to see some of the general steps that the
clinician followed during dream interpretation:
-
He commented on specific items in the dream and tried to relate those
items to possible feelings that the participant might have. In the example,
the specific items of the mountain walking and the chilly day were related
to the possible feelings about its being a cold experience.
-
He tried to induce the participant to agree with and expand on his
interpretation.
-
He provided a global interpretation of the dream's meaning. In the
example, the clinician suggested that possibly the participant was not
totally happy with himself, needed challenge, resisted help, and so forth.
-
He suggested the possibility that specific events of childhood are
commonly associated with dream reports like the one provided by the
participant. In the example, the specific events were getting lost and
feeling abandoned-in other words, the critical events used in this study for
all participants.
-
He explicitly suggested that such events had happened to the participant,
and he asked for the participant's agreement with that suggestion.
-
When the participant did not recall such an event, the clinician
explained that unpleasant childhood experiences can be buried and remain
unremembered but are often revealed in dreams.
The entire dream session lasted approximately 30 min. At the end of the dream
session, the clinician asked the participant to think over the proposed events
and to return later for the sleep assessment. These participants eventually
returned to participate in a subsequent sleep study that was actually totally
unrelated to the current experiment.
The initial experimenter, who had previously administered the LEI (hereafter
referred to as LEI-1), then contacted the participants in the dream condition
and arranged for them to return for a second administration of the LEI
(hereafter referred to as LEI-2). Approximately 10-15 days passed between LEI-1
and dream interpretation, and an additional 10-15 days passed between dream
interpretation and LEI-2. For the non-dream condition participants, the LEI
administrations were separated by the same amount of time but without any
intervening dream interpretation.
After the LEI-2, participants were thoroughly debriefed. At this time, they
were asked whether they had linked the two experiments in any way, and no
participant reported having done so.
To determine if the false dream interpretation had caused participants to
become more confident that the critical events had occurred, we examined whether
LEI scores moved up or down for each of the three critical items. We also
calculated the percentage of participants whose responses increased, decreased,
or did not change from the LEI-1 to the LEI-2. The data for the three critical
items (lost in public place, abandoned by parents, and lonely and lost) are
shown in Figure 1 . We predicted that after dream
interpretation, participants would be more confident that the events had
happened.
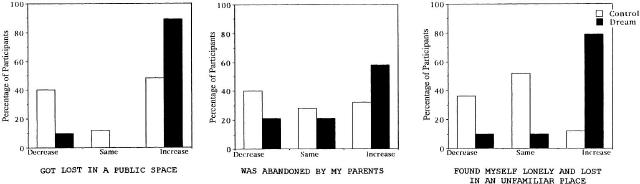
Figure 1. Percentage of participants who decreased, who stayed the same, and
who increased their scores for each of the three critical items on the Life
Events Inventory.
First examine what happened without dream interpretation: These participants
in the control condition reported no change in score on two target items and a
clear decrease on the remaining item ("lonely and lost"). The same was
not true for participants in the dream condition. For all three items, their
scores were far more likely to increase, and they rarely decreased on the LEI-2.
For two of the critical events, about 80% of the scores increased. To analyze
these data statistically, we conducted several Mann-Whitney U tests,
comparing the dream and non-dream (control) conditions. We found that the two
groups differed significantly for two of the critical items: "lost in a
public place" and "lonely and lost in an unfamiliar place."
Participants in the dream condition were far more likely to increase their
confidence that they had had these experiences before the age of 3 years.
The same differences between the dream and non-dream condition groups were
found when we analyzed the degree of movement. For each participant, we
calculated the numerical difference between the scores assigned to each item in
LEI-2 and the scores assigned to the same items in LEI-1. Figure
2 shows the change scores from LEI-1 to LEI-2 for the three critical items
for non-dream condition versus dream condition participants.
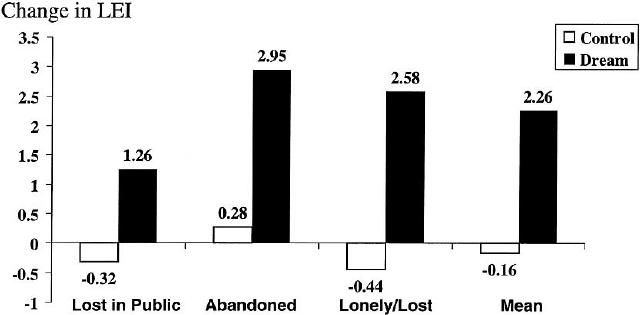
Figure 2. Mean change in scores on the Life Events Inventory (LEI) for each
of the three critical items. At the right is mean change collapsed across the
three critical items.
As Figure 2 shows, for control condition participants,
the changes in LEI scores were relatively small and not systematic. One item
changed in a slightly positive way ("abandoned by parents"), whereas
the other two items changed in a slightly negative way.
For the dream condition participants, the picture was completely different.
All three items changed in a positive direction. The biggest difference between
dream and non-dream condition participants occurred for the item "lonely
and lost in an unfamiliar place," where the dream condition participants
showed a mean positive change of 2.58 and the control participants showed a mean
negative change of -.44. At the right of Figure 2 , the mean
change in LEI is averaged across all critical items and participants, and a
strong overall influence of the dream interpretation can be seen. The mean
change in the dream condition was 2.26 on the 8-point scale, whereas in the
non-dream condition it was -.16.
To analyze these data statistically, we conducted several students' t tests
for independent samples on the change scores. We found that the dream and
non-dream condition participants differed significantly for two critical items:
lost in a public place and lonely and lost. Dream and non-dream participants
differed on the last critical item, abandoned by parents, only by a one-tailed
test. Thus, the two methods of analysis, one that involved proportions of
participants who shifted and one that involved measures of mean shift, produced
similar results.
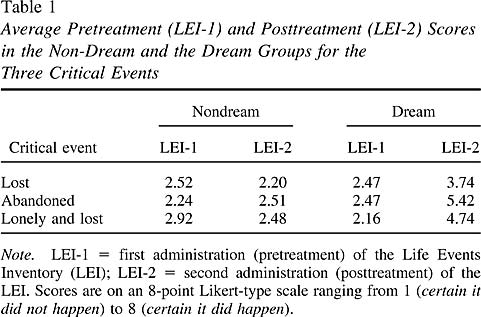
To be sure that our results were not due to inadvertent differences in
pretreatment LEI scores, we calculated the mean pretreatment score for each
critical item. These pretreatment scores are shown in Table 1 ,
separately for dream and non-dream participants. The posttreatment mean scores
are also shown. Notice that the dream and non-dream participants did not differ
in terms of their pretreatment scores, but they showed large differences in
their posttreatment scores.
The previous two analyses suggested that the dream manipulation caused
participants to become more certain that they had had specific negative
experiences in their early childhood. A question then arose as to whether the
shifts were localized only to the specific experiences mentioned by the
clinician, or whether the clinician's intervention caused a general negative
feeling, creating in participants the belief that they were more likely to have
experienced a vast array of negative events in their early lives. We assessed
this possibility by examining the dream condition versus non-dream condition
differences on the negative filler items, such as "witnessed a person
dying" or "threatened by a stranger." If the dream manipulation
produced general negativity, this negativity might be represented in increased
confidence on negative filler items as compared with non-dream condition
responses on those negative filler items. In fact, we found that the dream
manipulation had no impact on the negative filler items. Rather, the influence
of the dream manipulation was very specific to the critical items that were
specifically mentioned by the clinician.
Why did the dream interpretation lead to increased confidence that certain
suggested events occurred? One possible explanation is that the dream
interpretation created a true belief, reminding some participants of a true
experience from their past. Such a reminder, if it occurred, probably did not
occur during the therapy session itself, because no participant reported a
memory for one of the critical events during the therapy. However, in the 10-15
days between the therapy and the final session, some participants might have
recalled an actual experience. We deliberately suggested critical events to have
occurred before the age of 3 years so that any memory that was produced could be
deemed unlikely to be a real memory because of the childhood amnesia problem.
However, it is entirely possible that the therapy might have led to ruminations
that reminded participants of an event that occurred after the age of 3 years,
but they misdated the experience during LEI-2 and mistakenly thought that it
occurred before the age of 3. This process would lead to dramatic shifts in the
LEI. Our data cannot rule this possibility out completely, and it is possible
that these kinds of cases accounted for some of the shift that we observed.
However, we would argue that if participants were so ready to conclude after
dream interpretation that an experience that they actually had at age 6 or 8 or
12 happened to them before the age of 3, this also would constitute a distortion
of belief or memory.
Another possible reason that participants increased their confidence in the
suggested events is that the dream interpretation created a false belief. If
false beliefs have been constructed, how and why does this process happen? One
answer to this question can be found in the large literature on memory
distortion that has shown that people are susceptible to suggestion ( Gheorghiu,
Netter, Eysenck, & Rosenthal, 1989 ). In the current empirical work, we
have found a form of suggestion that is both explicit and subtle. It is explicit
in that the clinician used his authority to tell the dreamers that their mental
products were likely to be revealing particular past experiences. It is subtle
in the sense that the dreamers were encouraged to come up with their own
specific instances of such experiences.
Implications and Applications
Our findings have important implications for therapists. They show that
people are suggestible in a simulation that bears more resemblance to a
therapeutic setting than has been used in prior empirical studies. Moreover, the
findings hint at the strong influence that a clinician can have in a short
period of time. This power may extend to other therapist-client interactions
that are characterized by therapist interpretation of information provided by
the client.
One might ask whether it is reasonable to generalize from our brief therapy
simulation with students to the world of clinicians and their patients. After
all, many of the differences between our minitherapy and real-world therapy are
relatively easy to point out. Nonetheless, we believe that these very
differences are such that we may be underestimating the power and influence that
can occur in a clinical setting. We used students, who were presumably
reasonably mentally healthy, whereas clinical patients may have a greater need
to find an explanation for problems or distress. We had a single short therapy
simulation, whereas clinical patients often experience many sessions during
which suggested interpretations are offered to them. Our therapy simulation was
limited to only a few elements that the participants provided (e.g., the dream
and a brief reaction to the dream), whereas clinical patients provide a great
many elements (dreams, thoughts, behaviors, feelings) with which the therapist
works. Whether these elements are critical for influencing how people reflect on
their past experiences is, of course, a matter for further research
investigation.
One might ask whether it is even the case that therapists are using dream
material to suggest that events occurred in a client's early life. We have found
a number of examples that support the contention that some therapists do indeed
make these kinds of suggestions from dream material. This conclusion comes not
only from surveys of clinicians (e.g., Poole et al., 1995 ),
but also from the writings of specific clinicians. For example, in Crisis
Dreaming, readers are told, "Recurring dreams, particularly of being
chased or attacked, suggest that such events really occurred" ( Cartwright
& Lamberg, 1992 , p. 185). Are the authors of this book communicating
this information to their clients? Are therapist-readers of this book taking
dream material that involves chases and attacks and telling a client that it
means that such events occurred? Although we cannot know that therapist-readers
are following the advice implicit in this book, it is worth considering the
likelihood that they might do so and might inadvertently create false beliefs or
memories.
Could therapists produce similar effects without explicit dream
interpretation? We believe the dream interpretation is probably not necessary
but might add a bit of influential power. Here is why: Suppose instead of
interpreting dreams the clinician simply responds to the comments made by a
client during the first 5 min of interaction. If the clinician takes that 5 min
of material and interprets the material as being indicative of an early
childhood trauma, the client may eventually come to believe that he or she
experienced such a trauma. In fact, even in the absence of dream interpretation,
such suggestive comments might increase the likelihood of illusory beliefs or
memories. According to Lindsay and Read (1995) , suggestions
from a trusted authority can be especially influential when they communicate a
rationale for the plausibility of buried memories of childhood trauma. Moreover,
the trusted authority might be especially influential if he or she offers
repeated suggestions, giving anecdotes ostensibly from other patients.
However, it is also worth pointing out that working with dream material might
be a particularly potent way to influence clients, for better or worse. It
certainly might help to enhance the influence process, because people presumably
enter therapy with a set of beliefs about the meaning of dreams in their lives
and how much dreams can reveal about an individual's past. Given a
predisposition on the part of some clients to already believe in the
significance of dreams, the trusted authority can capitalize on the a priori
beliefs and use them in the service of altering the autobiography.
Are therapists aware of the power they have? Almost by definition therapists
must believe that they have the power to change people, because at least some
forms of therapy emphasize changing people's beliefs from ones that are
nonadaptive to ones that are more adaptive. Even more generally, therapy is
about changing people. However, therapists may be appreciating their power to
change people primarily when they are thinking about the good it can produce in
people or thinking about ways to make their clients change for the better. They
may not be appreciating that they also have the power to change people for the
worse. This type of change can happen, for example, when a therapist adopts a
hypothesis too early and, even when the hypothesis is wrong, presses it on the
client. Our data show that even a randomly generated hypothesis can be embraced
by individuals and can produce profound changes in the way they view their past.
We have demonstrated that these interventions can make people believe that they
have had experiences that they previously denied. However, it is also likely
that these interventions have the power to make people doubt their true
experiences. Our hope is that heightened awareness of this power might enhance
the likelihood of cautious use of these sorts of interventions.
References
Brenneis,C. B. (1997). Recovered memories of trauma:
Transferring the present to the past. Madison, WI: International
Universities Press.
Cartwright,R. & Lamberg,L. (1992). Crisis dreaming-Using
your dreams to solve your problems. New York: HarperCollins.
Fredrickson,R. (1992). Repressed memories. New York:
Simon & Schuster.
Freud,S. (1953). The interpretation of dreams (Standard
ed. 4 & 5). London: Hogarth Press. (Original work published 1900)
Freud,S. (1955). From the history of an infantile neurosis (standard
ed. 17, pp. 1-122). London: Hogarth Press. (Original work published 1918)
Gheorghiu,V. A., Netter,P., Eysenck,H. J. & Rosenthal,R.
(1989). Suggestion and suggestibility. New York: Springer-Verlag.
Lindsay,D. S. & Read,J. D. (1995). "Memory work"
and recovered memories of childhood sexual abuse: Scientific evidence and
public, professional, and personal issues. Psychology, Public Policy, &
the Law, 1 846-908.
Mazzoni,G. A. L. & Loftus,E. F. (1996). When dreams become
reality. Consciousness & Cognition, 5 442-462.
Polusny,M. A. & Follette,V. M. (1996). Remembering
childhood sexual abuse. , 27 41-52.
Poole,D. A., Lindsay,D. S., Memon,A. & Bull,R. (1995).
Psychotherapy and the recovery of memories of childhood sexual abuse: U.S. and
British practitioners' opinions, practices, and experiences. Journal of
Consulting and Clinical Psychology, 63 426-437.
van der Kolk,B., Britz,R., Burr,W., Sherry,S. & Hartmann,E.
(1984). Nightmares and trauma: A comparison of nightmares after combat with
life-long nightmares in veterans. , 141 187-190.
Wetzler,S. E. & Sweeney,J. A. (1986). Childhood amnesia:
An empirical demonstration. In D. C. Rubin (Ed.), Autobiographical memory (pp.
191-201). Cambridge, MA: Cambridge University Press.
Back to
Elizabeth Loftus homepage
|