Figure 1
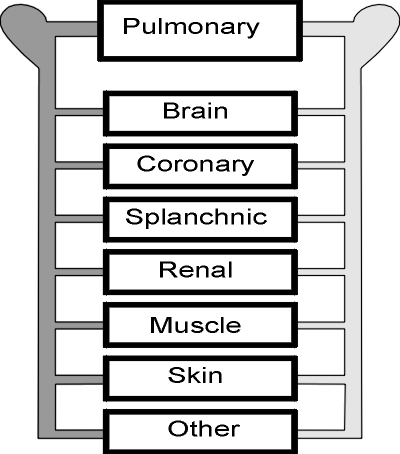
The distribution of the cardiac output among the organ vasculatures determines the convective distribution of heat within the body. Brain, coronary, splanchnic and renal vasculatures receive, altogether roughly 70% of the cardiac output in a healthy person at rest (11). High blood flow rate per unit mass in these organs and in the lungs results in small differences between their arterial and venous temperatures and rapid response of intra-organ temperatures to changes in arterial temperature. Altogether, these organs and the lungs can be regarded as a single thermal compartment in which temperatures are nearly identical to temperature in the pulmonary artery, Tpa The reductions in cardiac ouput and organ blood flow that occur in chronic heart failure may result in somewhat higher temperatures in the organs, relative to Tpa, and slower responses of organ temperatures to changes in thermal balance that alter Tpa.
The vasculature of skeletal muscle in a resting person receives a large fraction of the cardiac output, typically 18 % (11) but the perfusion rate per unit mass of muscle is so low that intramuscular temperatures are influenced by conductive heat exchange In chronic heart failure, minimal levels of blood flow and the higher surface:volume ratio of the wasted muscle mass are factors likely to result in lower muscle temperatures in environments that are neutral or only mildly cool for healthy persons. The inevitable increase in blood flow that accompanies activation of skeletal muscle even in the mild levels of exercise possible in chronic heart failure results in a rapid transfer of heat from the body core to the active muscle with associated rapid reduction of core temperature.
The cutaneous vasculature receives a variable fraction of the cardiac output, regulated according to thermoregulatory reflexes. Flow per unit mass can fall to the minimum required for metabolism, 1 or 2 ml/min per 100g of skin, in response to low skin and/or core temperatures. In the neutral range of skin temperatures, modulation of flow between this minimal level and the upper limit possible through release of vasoconstriction suffices for adjusting body heat loss to balance heat production and maintain normal core temperature. This range of flow is of little consequence as a cardiac stress, amounting at the most to only a few hundred ml/min. However, skin temperatures above the neutral range result in enormous increase in cutaneous vascular conductance. The reflex response to hyperthermia includes activation of a vasodilator system in skin that has been observed to result in cardiac output increase in hyperthermic healthy young men in excess of 7 liters/min. Direct application of heat to the skin has a similar dilator effect. Even though these vascular changes in the skin may be inhibited in chronic heart failure, they undoubtedly have the potential for major reduction of total peripheral resistance.
The box labeled "other" represents the vasculatures that receive the remainder of the cardiac ouput, roughly 5% in a resting person (11). These include the circulation of a major fraction of body mass, the skeleton, thermally important as source or sink of heat (with slow dynamics), and fat, thermally important as an insulating layer.